Placental abruption
Overview
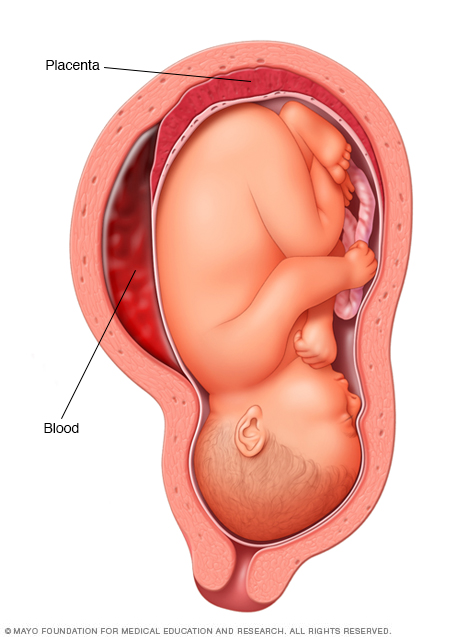
The placenta is an organ that develops in the uterus during pregnancy. Placental abruption occurs when the placenta separates from the inner wall of the uterus before birth. Placental abruption can deprive the baby of oxygen and nutrients and cause heavy bleeding in the mother. In some cases, early delivery is needed.
Placental abruption (abruptio placentae) is an uncommon yet serious complication of pregnancy. The placenta develops in the uterus during pregnancy. It attaches to the wall of the uterus and supplies the baby with nutrients and oxygen.
Placental abruption occurs when the placenta partly or completely separates from the inner wall of the uterus before delivery. This can decrease or block the baby's supply of oxygen and nutrients and cause heavy bleeding in the mother.
Placental abruption often happens suddenly. Left untreated, it endangers both the mother and the baby.
Symptoms
Placental abruption is most likely to occur in the last trimester of pregnancy, especially in the last few weeks before birth. Signs and symptoms of placental abruption include:
- Vaginal bleeding, although there might not be any
- Abdominal pain
- Back pain
- Uterine tenderness or rigidity
- Uterine contractions, often coming one right after another
Abdominal pain and back pain often begin suddenly. The amount of vaginal bleeding can vary greatly, and doesn't necessarily indicate how much of the placenta has separated from the uterus. It's possible for the blood to become trapped inside the uterus, so even with a severe placental abruption, there might be no visible bleeding.
In some cases, placental abruption develops slowly (chronic abruption), which can cause light, intermittent vaginal bleeding. Your baby might not grow as quickly as expected, and you might have low amniotic fluid or other complications.
When to see a doctor
Seek emergency care if you have signs or symptoms of placental abruption.
Causes
The cause of placental abruption is often unknown. Possible causes include trauma or injury to the abdomen — from an auto accident or fall, for example — or rapid loss of the fluid that surrounds and cushions the baby in the uterus (amniotic fluid).
Risk factors
Factors that can increase the risk of placental abruption include:
- Placental abruption in a previous pregnancy that wasn't caused by abdominal trauma
- Chronic high blood pressure (hypertension)
- Hypertension-related problems during pregnancy, including preeclampsia, HELLP syndrome or eclampsia
- A fall or other type of blow to the abdomen
- Smoking
- Cocaine use during pregnancy
- Early rupture of membranes, which causes leaking amniotic fluid before the end of pregnancy
- Infection inside of the uterus during pregnancy (chorioamnionitis)
- Being older, especially older than 40
Complications
Placental abruption can cause life-threatening problems for both mother and baby.
For the mother, placental abruption can lead to:
- Shock due to blood loss
- Blood clotting problems
- The need for a blood transfusion
- Failure of the kidneys or other organs resulting from blood loss
- Rarely, the need for hysterectomy, if uterine bleeding can't be controlled
For the baby, placental abruption can lead to:
- Restricted growth from not getting enough nutrients
- Not getting enough oxygen
- Premature birth
- Stillbirth
Prevention
You can't prevent placental abruption, but you can decrease certain risk factors. For example, don't smoke or use illegal drugs, such as cocaine. If you have high blood pressure, work with your health care provider to monitor the condition.
Always wear your seatbelt when in a motor vehicle. If you've had abdominal trauma — from an auto accident, fall or other injury — seek immediate medical help.
If you've had a placental abruption, and you're planning another pregnancy, talk to your health care provider before you conceive to see if there are ways to reduce the risk of another abruption.
Diagnosis
If your health care provider suspects placental abruption, he or she will do a physical exam to check for uterine tenderness or rigidity. To help identify possible sources of vaginal bleeding, your provider will likely recommend blood and urine tests and ultrasound.
During an ultrasound, high-frequency sound waves create an image of your uterus on a monitor. It's not always possible to see a placental abruption on an ultrasound, however.
Treatment
It isn't possible to reattach a placenta that's separated from the wall of the uterus. Treatment options for placental abruption depend on the circumstances:
The baby isn't close to full term. If the abruption seems mild, your baby's heart rate is normal and it's too early for the baby to be born, you might be hospitalized for close monitoring. If the bleeding stops and your baby's condition is stable, you might be able to rest at home.
You might be given medication to help your baby's lungs mature and to protect the baby's brain, in case early delivery becomes necessary.
- The baby is close to full term. Generally after 34 weeks of pregnancy, if the placental abruption seems minimal, a closely monitored vaginal delivery might be possible. If the abruption worsens or jeopardizes your or your baby's health, you'll need an immediate delivery — usually by C-section.
For severe bleeding, you might need a blood transfusion.
Preparing for an appointment
Placental abruption is often a medical emergency, leaving you no time to prepare. However, it's possible that your health care provider might notice signs of a coming abruption.
Depending on the suspected severity of your placental abruption, you might be admitted to the hospital and monitored. Or you might be admitted for emergency surgery to deliver the baby.
If you and the baby are being monitored in the hospital, here's some information to help you prepare for what's to come.
What you can do
While you're in the hospital:
- Pay attention to changes. Alert your health care team immediately if there's a change in your symptoms or their frequency.
- Let your doctor know about all medications you've been taking, including vitamins and supplements. Include whether you've smoked during your pregnancy or used illegal drugs.
- Ask a loved one or friend to be with you, if possible. Someone who's with you can help you remember the information provided, especially in an emergency.
Some questions you might want to ask your doctor include:
- What tests do I need?
- Is the baby in danger? Am I?
- What are the treatment options?
- What are the possible complications?
- What can I expect if the baby is born now?
- Will I need a blood transfusion?
- What are the chances of my needing a hysterectomy after the delivery?
What to expect from your doctor
Your doctor is likely to ask you questions, including:
- When did your signs and symptoms begin?
- Have you noticed changes in your signs and symptoms?
- How much bleeding have you noticed?
- Can you feel your baby moving?
- Have you noticed clear fluid leaking from your vagina?
- Have you had nausea, vomiting or lightheadedness?
- Are you having contractions? If so, how close together are they?
Content Last Updated: January 18, 2020
Content provided by Mayo Clinic ©1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use