Stereotactic radiosurgery
Overview
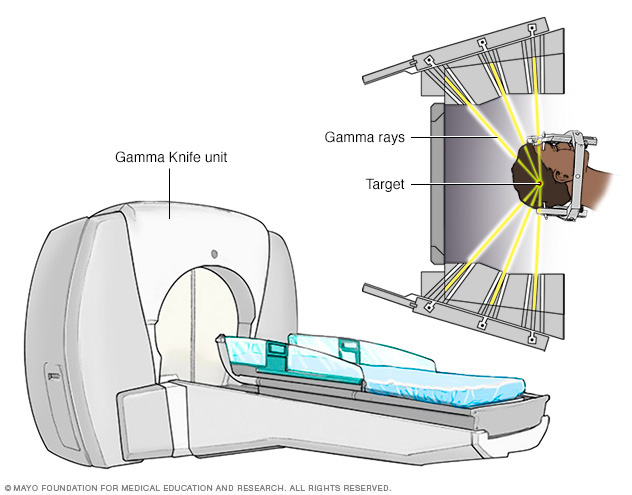
Gamma Knife stereotactic radiosurgery technology uses many small gamma rays to deliver a precise dose of radiation to a target.
Stereotactic radiosurgery (SRS) uses many precisely focused radiation beams to treat tumors and other problems in the brain, neck, lungs, liver, spine and other parts of the body.
It is not surgery in the traditional sense because there's no incision. Instead, stereotactic radiosurgery uses 3D imaging to target high doses of radiation to the affected area with minimal impact on the surrounding healthy tissue.
Like other forms of radiation, stereotactic radiosurgery works by damaging the DNA of the targeted cells. The affected cells then lose the ability to reproduce, which causes tumors to shrink.
Stereotactic radiosurgery of the brain and spine is typically completed in a single session. Body radiosurgery is used to treat lung, liver, adrenal and other soft tissue tumors, and treatment typically involves multiple (three to five) sessions.
When doctors use stereotactic radiosurgery to treat tumors in areas of the body other than the brain, it's sometimes called stereotactic body radiotherapy (SBRT) or stereotactic ablative radiotherapy (SABR).
Doctors use three types of technology to deliver radiation during stereotactic radiosurgery in the brain and other parts of the body:
- Linear accelerator (LINAC) machines use X-rays (photons) to treat cancerous and noncancerous abnormalities in the brain and other parts of the body. LINAC machines are also known by the brand name of the manufacturer, such as CyberKnife and TrueBeam. These machines can perform stereotactic radiosurgery (SRS) in a single session or over three to five sessions for larger tumors, which is called fractionated stereotactic radiotherapy.
- Gamma Knife machines use 192 or 201 small beams of gamma rays to target and treat cancerous and noncancerous brain abnormalities. Gamma Knife machines are less common than LINAC machines and are used primarily for small to medium tumors and lesions in the brain associated with a variety of conditions.
- Proton beam therapy (charged particle radiosurgery) is the newest type of stereotactic radiosurgery and is available in only a few research centers in the U.S, although the number of centers offering proton beam therapy has greatly increased in the last few years. Proton beam therapy can treat brain cancers in a single session using stereotactic radiosurgery, or it can use fractionated stereotactic radiotherapy to treat body tumors over several sessions.
How it works
All types of stereotactic radiosurgery and radiotherapy work in a similar manner.
The specialized equipment focuses many small beams of radiation on a tumor or other target. Each beam has very little effect on the tissue it passes through, but a targeted dose of radiation is delivered to the site where all the beams intersect.
The high dose of radiation delivered to the affected area causes tumors to shrink and blood vessels to close off over time following treatment, robbing the tumor of its blood supply.
The precision of stereotactic radiosurgery means there's minimal damage to the healthy surrounding tissues. In most cases, radiosurgery has a lower risk of side effects compared with other types of traditional surgery or radiation therapy.
Why it's done
Around 50 years ago, stereotactic radiosurgery was pioneered as a less invasive and safer alternative to standard brain surgery (neurosurgery), which requires incisions in the skin, skull, and membranes surrounding the brain and brain tissue.
Since then, the use of stereotactic radiosurgery has expanded widely to treat a variety of neurological and other conditions, including:
-
Brain tumor. Stereotactic radiosurgery, such as Gamma Knife, is often used to treat noncancerous (benign) and cancerous (malignant) brain tumors, including meningioma, paraganglioma, hemangioblastoma and craniopharyngioma.
SRSmay also be used to treat cancers that have spread to the brain from other parts of the body (brain metastases).
-
Arteriovenous malformation (AVM). AVMs are abnormal tangles of arteries and veins in your brain. In an AVM, blood flows directly from your arteries to veins, bypassing smaller blood vessels (capillaries). AVMs may disrupt the normal flow of blood and lead to bleeding (hemorrhage) or stroke.
Stereotactic radiosurgery destroys the AVM and causes the affected blood vessels to close off over time.
-
Trigeminal neuralgia. Trigeminal neuralgia is a chronic pain disorder of one or both of the trigeminal nerves, which relay sensory information between your brain and areas of your forehead, cheek and lower jaw. This nerve disorder causes extreme facial pain that feels like an electric shock.
Stereotactic radiosurgery treatment for trigeminal neuralgia targets the nerve root to disrupt these pain signals.
-
Acoustic neuroma. An acoustic neuroma (vestibular schwannoma), is a noncancerous tumor that develops along the main balance and hearing nerve leading from your inner ear to your brain.
When the tumor puts pressure on the nerve, a person can experience hearing loss, dizziness, loss of balance and ringing in the ear (tinnitus). As the tumor grows, it can also put pressure on the nerves affecting sensations and muscle movement in the face.
Stereotactic radiosurgery may stop the growth or minimize the size of an acoustic neuroma with little risk of permanent nerve damage.
-
Pituitary tumors. Tumors of the bean-sized gland at the base of the brain (pituitary gland) can cause a variety of problems. The pituitary gland controls hormones in your body that control various functions, such as your stress response, metabolism, growth and sexual function.
Radiosurgery can be used to shrink the tumor and lessen the disruption of pituitary hormone regulation.
- Tremors. Stereotactic radiosurgery may be used to treat tremors associated with functional neurological disorders such as Parkinson's disease and essential tremor.
- Other cancers. SRS may be used to treat cancers of the liver, lung and spine.
Researchers are also exploring the use of stereotactic radiosurgery to treat other conditions, including melanoma of the eye, breast cancer, lung cancer, prostate cancer, epilepsy and psychological disorders such as obsessive-compulsive disorder.
Risks
Stereotactic radiosurgery doesn't involve surgical incisions, so it's generally less risky than traditional surgery. In traditional surgery, you may have risks of complications with anesthesia, bleeding and infection.
Early complications or side effects are usually temporary. They may include:
- Fatigue. Tiredness and fatigue may occur for the first few weeks after stereotactic radiosurgery.
- Swelling. Swelling in the brain at or near the treatment site can cause signs and symptoms such as headache, nausea and vomiting. Your doctor may prescribe anti-inflammatory medications (corticosteroid medications) to prevent such problems or to treat symptoms if they appear.
- Scalp and hair problems. Your scalp may be red, irritated or sensitive at sites where a device is attached to your head during the treatment. Some people temporarily lose a small amount of hair.
Rarely, people may experience late side effects, such as other brain or neurological problems, months after treatment.
How you prepare
Preparation for stereotactic radiosurgery and stereotactic body radiotherapy may vary depending on the condition and body area being treated but usually involves the following steps:
Food and medications
- Don't eat or drink anything after midnight the night before the procedure.
- Talk to your doctor about whether you can take your regular medications the night before or morning of the procedure.
Clothing and personal items
Wear comfortable, loosefitting clothing.
Avoid wearing the following items during SRS of the brain or spine:
- Jewelry
- Eyeglasses
- Contact lenses
- Makeup
- Nail polish
- Dentures
- Wigs or hairpieces
Precautions regarding medications and allergies
Tell your doctor if you:
- Are taking pills or injections to control diabetes.
- Are allergic to shellfish or iodine, which are chemically related to special dyes that may be used during the procedure.
- Have implanted medical devices in your body, such as a pacemaker, artificial heart valve, aneurysm clips, neurostimulators or stents.
Bring any medications you are currently taking with you to the treatment center and ask about what you should do about taking your medications on the day of the procedure.
What you can expect

Stereotactic radiosurgery is usually an outpatient procedure, but the entire process will take most of a day. You may be advised to have a family member or friend who can be with you during the day and who can take you home.
You may have a tube that delivers fluids to your blood stream (intravenous, or IV, line) to keep you hydrated during the day if you are not allowed to eat or drink during the procedure. A needle at the end of the IV is placed in a vein, most likely in your arm.
Before the procedure
The steps immediately prior to treatment may vary depending on the location of your treatment area and the type of equipment being used to deliver the radiation.
Preparation for Gamma Knife and LINAC stereotactic radiosurgery of the brain is very similar (except for the first step — a head frame is not needed for LINAC stereotactic radiosurgery) and involves three steps:
-
Head frame placement. Before the procedure begins, you'll have a lightweight frame attached to your head with four pins. This frame will stabilize your head during the radiation treatment and serve as a point of reference for focusing the beams of radiation. Some types of brain radiosurgery may not require head frame placement.
If a head frame is required, you'll receive numbing shots in the four places on your scalp where the pins will be inserted — two points on your forehead and two at the back of your head. Your hair will not be shaved, and you may be given a special shampoo to cleanse your scalp and help the frame stay in place.
You don't need a head frame with LINAC stereotactic radiosurgery of the brain. The radiosurgery typically can be delivered with a soft plastic mask that forms to your face. The advantage of this approach is it facilitates multiple (three to five) treatments and avoids the uncomfortableness of frame placement.
- Imaging. After the head frame is attached, you'll undergo imaging scans of your brain that show the location of the tumor or other abnormality in relation to the head frame. The type of scan used depends on the condition being treated:
-
Tumors. Imaging for tumors may include computerized tomography (CT) scan or magnetic resonance imaging (MRI). In a CT scan, a series of X-rays create a detailed image of your brain. In an MRI scan, a magnetic field and radio waves create detailed images of your brain.
Doctors may inject a dye into a blood vessel to view the blood vessels in your brain and highlight blood circulation. In some cases, you may have an MRI scan and a CT scan.
-
Arteriovenous malformations (AVMs). Imaging for brain AVMs may include CT scans, MRI scans, cerebral angiograms or some combination of these tests.
In a cerebral angiogram, a doctor inserts a small tube in a blood vessel in your groin and threads it to the brain using X-ray imaging. A doctor injects dye through the blood vessels to make them visible on X-rays. Your doctor may inject a dye into a blood vessel during CT or MRI scans to view the blood vessels and highlight blood circulation.
- Trigeminal neuralgia. An MRI or CT scan is used to create images of nerve fibers to select a target area for treating trigeminal neuralgia.
-
-
Dose planning. The results of the brain scans are fed into a computerized planning system that enables the radiosurgery team to plan the appropriate areas to treat, dosages of radiation and how to focus the radiation beams to treat the areas.
This planning process may take an hour or two. During that time, you can relax in another room, but the frame must remain attached to your head. If you are doing LINAC stereotactic radiosurgery of the brain, typically you would be sent home during the planning process and treatment would be delivered a few days later.
Preparation for stereotactic radiosurgery or radiotherapy for other parts of the body also involves several steps, including:
- Marking. Some SRS technologies require the placement of a fiducial marker in or near the tumor in certain cases. This procedure is usually done as an outpatient procedure prior to SRS treatment. But this step is not needed for most CT-guided technologies.
-
Simulation. A radiation oncologist will conduct a simulation to determine the best placement of your body to align it with the radiation beams. Your body will be held very tightly and still by an immobilization device. Tell your doctor if you have claustrophobia.
After you are immobilized, imaging scans will be taken, and you'll likely be sent home prior to the next stage.
- Planning. Using the imaging scans and specialized software, your treatment team will determine the best combination of radiation beams to target your tumor or other abnormality.
During the procedure
Children are often anesthetized for the imaging tests and during the radiosurgery. Adults are usually awake, but you may be given a mild sedative to help you relax.
If you are using a Gamma Knife machine, you'll lie on a bed that slides into the machine, and your head frame will be attached securely to the bed frame. The machine does not move during treatment; instead, the bed moves within the machine. The procedure may take less than an hour to about four hours, depending on the size and shape of the target. If treating with LINAC stereotactic radiosurgery of the brain the treatment will be quicker.
Unlike the Gamma Knife, the LINAC machine moves and rotates around the target during treatment to deliver radiation beams from different angles. The treatment takes less than an hour.
During the procedure:
- You won't feel the radiation.
- You'll be able to talk with the doctors via a microphone.
After the procedure
After the procedure, you can expect the following:
- The head frame, if used, will be removed. You may have minor bleeding or tenderness at the pin sites.
- If you experience headache, nausea or vomiting after the procedure, you'll receive appropriate medications.
- You'll be able to eat and drink after the procedure.
Results

Gamma Knife radiosurgery uses multiple, tiny beams of radiation to shrink tumors. The left brain scan shows a pretreatment image of a noncancerous tumor — an image enhanced by the use of a special dye (contrast agent). At six months after treatment (middle image), the tumor appears slightly larger but doesn't take up as much of the contrast agent — isn't as bright in the center — indicating a positive treatment effect. At seven years (right image), the tumor appears much smaller.
The treatment effect of stereotactic radiosurgery occurs gradually, depending on the condition being treated:
- Benign tumors (including vestibular schwannoma). Following stereotactic radiosurgery, the tumor may shrink over a period of 18 months to two years, but the main goal of treatment for benign tumors is to prevent any future tumor growth.
- Malignant tumors. Cancerous (malignant) tumors may shrink more rapidly, often within a few months.
- Arteriovenous malformations (AVMs). The radiation therapy causes the abnormal blood vessels of brain AVMs to thicken and close off. This process may take two years or more.
- Trigeminal neuralgia. SRS creates a lesion that blocks transmission of pain signals along the trigeminal nerve. Many people experience pain relief within several weeks, but it may take several months.
You'll receive instruction on appropriate follow-up exams to monitor your progress.
Content Last Updated: April 27, 2019
Content provided by Mayo Clinic ©1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use